
New Study Urges Earlier Detection of Valley Fever as Cases Climb


Key Points:
-
Valley fever is widely underdiagnosed and often mistaken for common respiratory illnesses, leading to delayed diagnosis and unnecessary antibiotic use.
-
Cases are rising and spreading geographically, driven by climate patterns, soil disruption and population growth, making the disease a growing public health concern.
-
The study promotes the COCCI framework, which emphasizes early testing, exposure assessment and structured clinical decision-making to improve outcomes and reduce complications.
A new study published in The Journal for Nurse Practitioners calls for a shift in how Valley fever is recognized and treated, warning that delayed diagnosis continues to prolong illness, drive unnecessary treatment and contribute to preventable deaths.
The paper was authored and led by Ayomidamope "Ayo" Adebiyi, DNP, a board-certified family nurse practitioner and clinical lead at UC Merced's Occupational Health Services department, and co-authored by Professor Mary K. Estrada at the University of Arizona. Adebiyi recently completed her Doctor of Nursing Practice with a focus on Executive Systems Leadership and Health Policy, and a post-master's certificate in Nursing Education, both at Johns Hopkins University.
The paper outlines a structured approach to help frontline providers identify the disease earlier — a step researchers say could significantly improve patient outcomes.
“Valley fever is an underdiagnosed but growing public health issue, especially in endemic regions,” the study noted, emphasizing that better awareness, earlier testing and consistent clinical practices are essential to reducing illness severity and healthcare costs.
“Eighty percent of people with Valley fever don’t get the correct diagnosis until a median of 23 days after their first clinical contact, if they even get tested. That’s a lot of illness, a lot of days lost from work and a lot of unnecessary antibiotics.”
Missed Diagnoses, Growing Burden
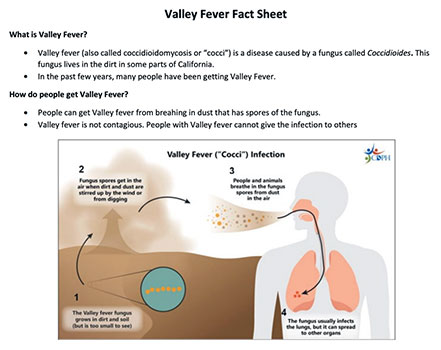
Valley fever, or coccidioidomycosis, is caused by inhaling fungal spores that live in soil. While once considered a regional illness concentrated in the southwestern United States, it has now expanded beyond traditional boundaries and affected far more people than reported data suggests.
Researchers estimate that between 205,000 and 360,000 symptomatic cases occur annually — far higher than official counts. A major challenge is delayed recognition, with many patients waiting weeks for an accurate diagnosis while often receiving ineffective antibiotics. Because symptoms such as fatigue, cough, fever and shortness of breath resemble more common respiratory illnesses, the infection is frequently overlooked in early stages.
“Eighty percent of people with Valley fever don’t get the correct diagnosis until a median of 23 days after their first clinical contact, if they even get tested,” Adebiyi said. “That’s a lot of illness, a lot of days lost from work and a lot of unnecessary antibiotics.”
Cases are Rising
Overlapping environmental and demographic changes drive the increase in Valley fever. Adebiyi pointed to climate patterns as a key factor, with longer droughts followed by rainfall disrupting soil and increasing the spread of airborne spores. At the same time, expanding development is increasing exposure.
“As rural areas are almost becoming semi-urban, there’s more construction, which disrupts the soil,” she said.
Improved reporting has made the disease more visible, though many cases still go undiagnosed when symptoms are mild or resolve on their own.
The result is a disease that is both expanding geographically and still widely underrecognized — especially in areas where clinicians may not routinely consider it.
At the center of the study is the COCCI framework, a clinical guide designed to help nurse practitioners and other providers identify Valley fever sooner and manage it appropriately:
- Consider exposure: Assess whether patients live in or have traveled to endemic areas or have been exposed to dust, construction or soil disturbance
- Order diagnostic testing early: Especially for patients with persistent respiratory symptoms or those who do not respond to initial treatment
- Check for risk factors: Identify patients at higher risk for severe disease, including those who are immunocompromised, pregnant or have underlying conditions
- Check for complications: Evaluate for signs of more serious disease, such as neurologic symptoms or widespread infection
- Initiate appropriate care: Manage uncomplicated cases in primary care and refer severe or complex cases to specialists
At its core, the COCCI framework shifts clinical thinking from “treat first, test later” to “evaluate exposure, test early and manage deliberately.” Rather than relying on intuition, the framework provides a clear, step-by-step approach.
A defining feature of the COCCI framework is reassessment after initial care. Clinicians are encouraged to schedule follow-up visits, monitor symptoms and adjust treatment if patients do not improve.
“Having this framework would really change outcomes. If we can quickly identify Valley fever, we can change the quality of life for many people and even save some lives.”
Lorena Anderson

Senior Writer and Public Information Representative
Office: (209) 228-4406
Mobile: (209) 201-6255